AXA Hong Kong, CUHK, and Oxford VR announce partnership to pilot VR immersive therapy.
In Hong Kong, 1 in 7 adults live with anxiety or depression - yet only 1 in 4 ever seeks help. The question this project asked: could immersive VR lower that barrier? My job was to make sure the product actually worked for the people it was designed for, before it reached them at scale.

Trying out Oxford VR's VR-enabled Social Avoidance treatment program.
The Challenge
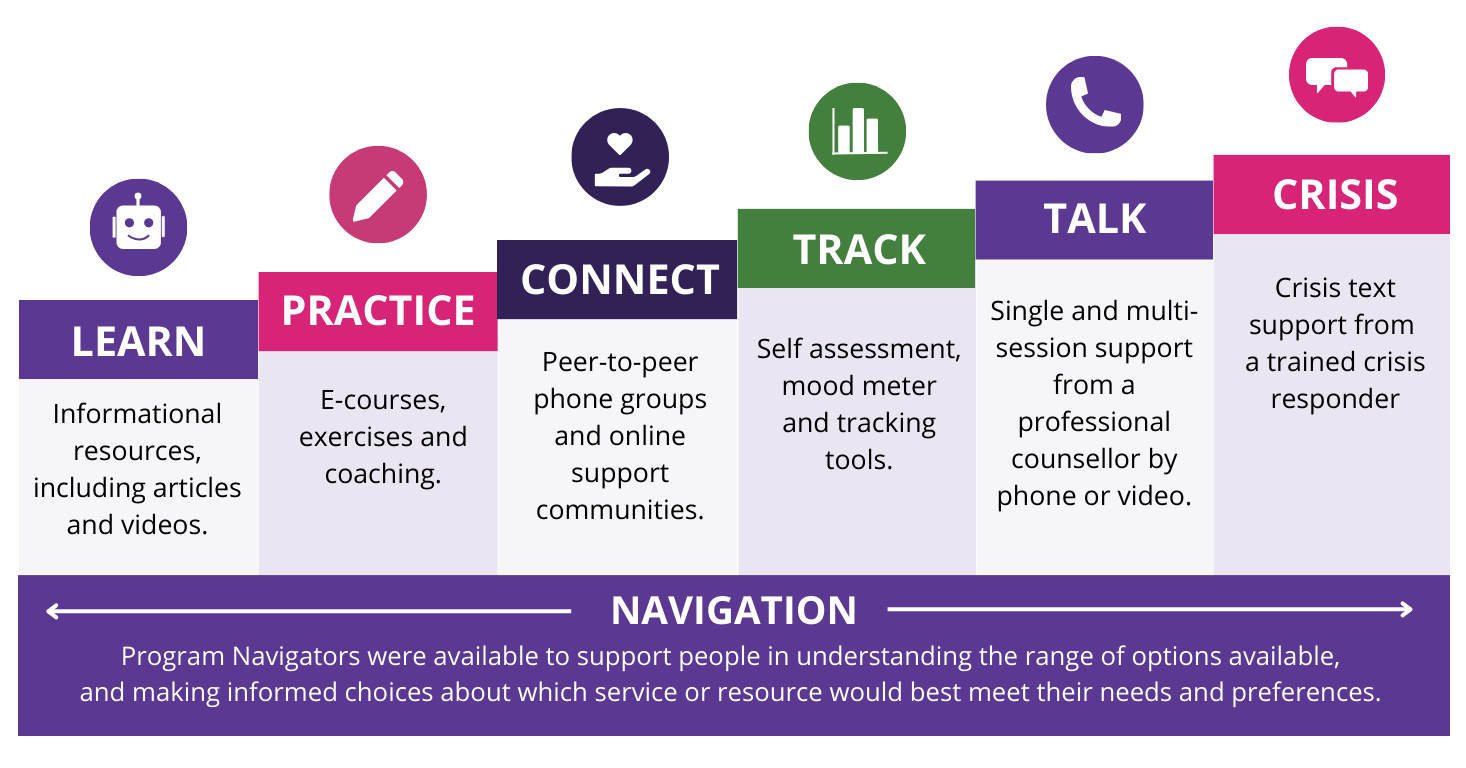
"Yes I Can" was a B2B VR therapy product developed in partnership between Oxford VR, CUHK, and AXA Hong Kong, designed to treat anxious social avoidance and delivered free to the public and AXA corporate customers as part of their employee mental health benefits. The product had clinical backing and an evidence base from Oxford. What it didn't yet have was localization that held up for Hong Kong users.
Before launch, the team needed to answer a question: does a VR therapy program designed in the UK actually trigger the right psychological responses in a Hong Kong context? Or does cultural mismatch quietly undermine the therapeutic effect?

Emma, the VR coach, guides users in confronting anxiety across different social scenarios.
What I Did
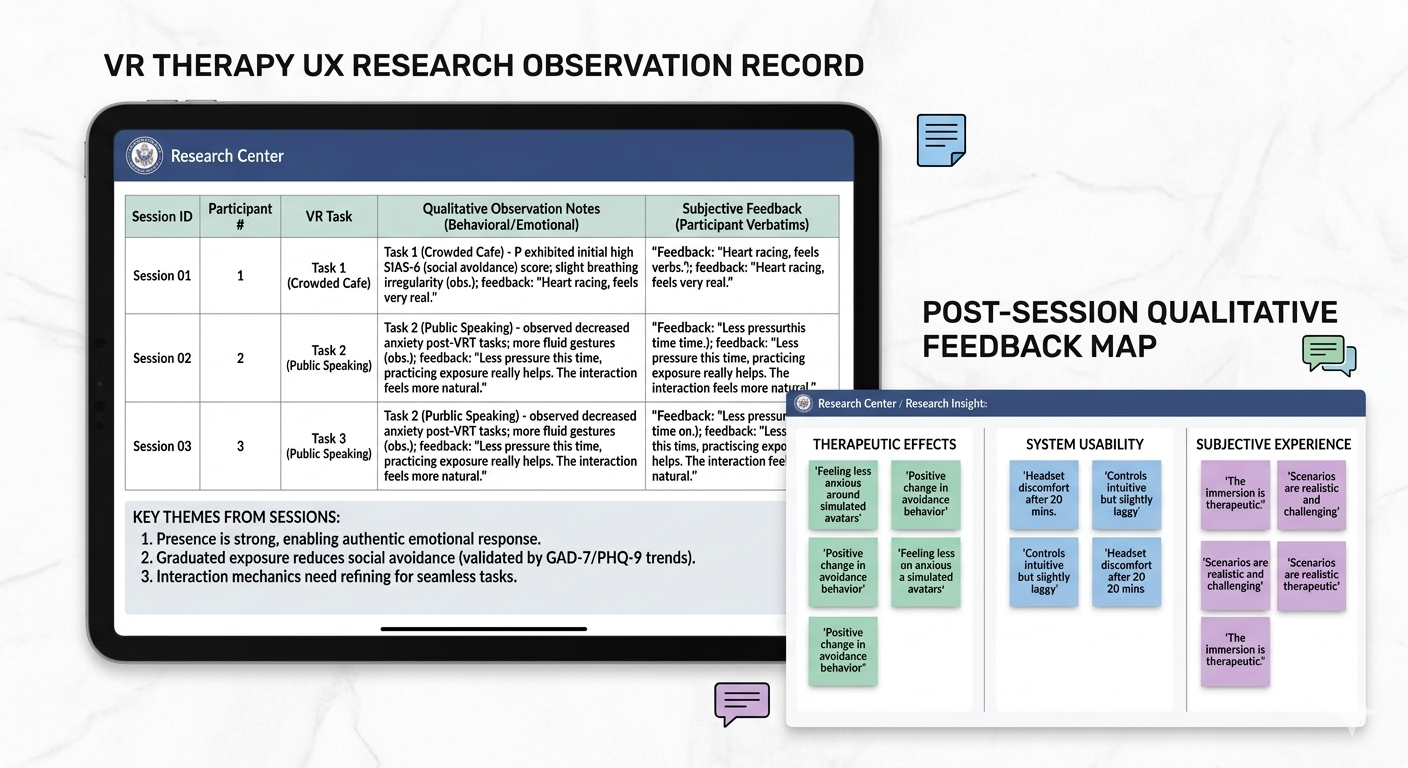
- Planned and executed usability testing sessions, including training team members on procedures to ensure consistency across sessions
- Administered validated clinical scales (GAD-7, PHQ-9, SIAS-6, Oxford Behavioral Avoidance Task) pre-, during, and post-session to measure actual symptom change, not just UX satisfaction
- Synthesized qualitative feedback and clinical data into prioritized, actionable recommendations for a cross-functional team spanning UK and HK
- Advocated for user needs in stakeholder reviews where the pressure was to ship, not iterate
Dockside perspective, capturing the soul of the water.
Key Decisions
- Escalated cultural realism as a product risk, not just a design note. Users reported that the social anxiety triggers in the original scenarios didn't match Hong Kong's context. The fear wasn't crowd density in the abstract, it was specific: uniformed police presence, a culturally loaded trigger that the UK-designed scenario hadn't accounted for. I framed this not as a localization preference but as a therapeutic validity issue: a VR exposure therapy that doesn't trigger the right anxiety can't reduce it. This required creating an additional scenario, which extended the development timeline. The alternative, shipping a product that didn't work for its target population, wasn't a viable tradeoff.
- Flagged broken feedback logic as a trust and safety issue. In the café scenario, the system responded with the same line regardless of user input, the VR environment wasn't actually listening. For a typical product this is a bug. For a therapeutic product where users are practising social interaction, it was more serious: if the environment doesn't respond authentically, users can't build real confidence from it. I prioritized this fix above visual improvements because it went to the core therapeutic mechanism.
- Pushed for a post-session reflection and take-home assignments. Users were completing VR sessions without any structure for applying what they'd practised to real life. The gap between in-headset behaviour and real-world generalisation is a gap in VR therapy, and the product wasn't addressing it. I recommended between-session assignments that mapped VR scenarios to equivalent real-world exposures. The tradeoff was added content design work. The outcome: measurably improved engagement between sessions and, more importantly, users beginning to attempt real-world situations they previously avoided.

Venice, and a moment between two.
Outcome
- Scenario difficulty and cultural triggers recalibrated for the Hong Kong context
- Sound detection and response logic corrected across all scenarios
- Take-home assignments added to bridge the gap between VR practice and daily life behaviour
- UK–HK product team misalignments surfaced and resolved before launch
- One participant reported attempting solo real-world activities for the first time — the intended clinical outcome of the therapy

A spontaneous rhythm, a shared moment, pure joy.
Key takeaways: In therapeutic products, realism isn't a visual design goal, it's a clinical requirement. Every inconsistency between what the VR environment promised and what it delivered undermined the mechanism of the therapy itself. Holding that standard, even when it created friction with the timeline, was the most important contribution I made on this project.